

Experimental Study on the Association Mechanism Between Liver Disease and Cardiac Function Based on Hemodynamics
-
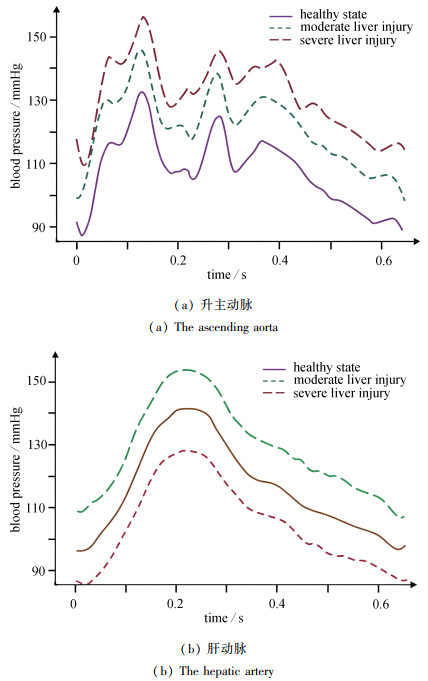
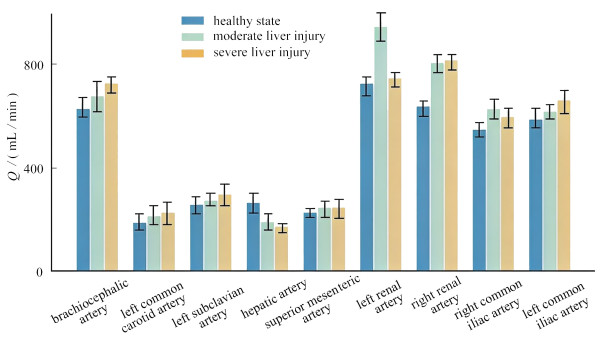
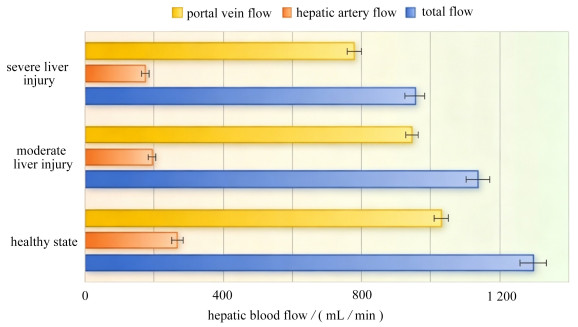
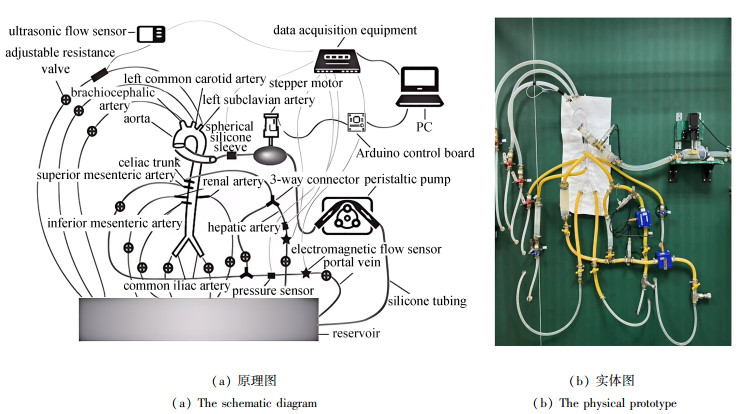
摘要: 非酒精性脂肪肝在全球范围内正日益发展成为流行的慢性肝病,尽管已有研究关注肝损伤与心脏功能障碍之间的关系,但其具体的影响机制仍未被充分阐明,血流动力学变化与心功能障碍联系紧密,可能是其中的关键影响因素. 以心血管系统的构造及生理功能为依据,搭建了体外模拟循环系统,并模拟各血流动力学参数. 进行分组实验,设定了健康、中度以及重度肝损伤这三种状态,每组均获取实时的压力与流量数据. 结果表明,随着肝损伤程度不断增加,升主动脉以及肝动脉的压力有所升高,在重度肝损伤的情况下,升主动脉压力与肝动脉压力峰值分别提升了25.7%和19.3%,谷值分别提升了49.7%和26.7%,同时平均门静脉压力也出现了大幅上升. 肝损伤状态下,血流会重新分配到动脉系统的其他分支,管径较大的血管流量提升较大,头臂动脉、右侧髂总动脉和右肾动脉的血流量分别提高约15%、12%和28%. 肝动脉与门静脉的流量同步下降,肝动脉流量对于总入肝流量的比例基本保持在20%. 讨论说明,肝损伤所产生的血流动力学环境变化为引发肝硬化心肌病等心功能障碍提供了相应依据,并且与传统代谢异常理论存在一定的互补关系. 研究结果为理解肝脏损伤引发心功能变化提供了血流动力学证据,有一定的临床指导意义.Abstract: The non-alcoholic fatty liver disease is increasingly becoming a prevalent chronic liver condition worldwide. Although previous studies have focused on the relationship between liver injury and cardiac dysfunction, the specific underlying mechanisms remain inadequately elucidated. Hemodynamic changes, which are closely linked to cardiac dysfunction, may be a key influencing factor. Based on the structure and physiological functions of the cardiovascular system, an in vitro simulated circulatory system was constructed to replicate various hemodynamic parameters. Grouped experiments were conducted, to simulating 3 states: healthy, moderate and severe liver injuries, with real-time pressure and flow data collected for each group. The results show that, as the liver injury degree increases, the pressure in the ascending aorta and hepatic artery will rise. In the case of severe liver injury, the peak pressures in the ascending aorta and hepatic artery will increase by 25.7% and 19.3%, respectively, while the trough pressures will increase by 49.7% and 26.7%, respectively. Additionally, the average portal vein pressure significantly increases. Under liver injury conditions, the blood flow will be redistributed to other branches of the arterial system, with larger-diameter vessels experiencing greater flow increases. The blood flow in the brachiocephalic artery, the right common iliac artery, and the right renal artery will increase by approximately 15%, 12%, and 28%, respectively. Meanwhile, the flow in the hepatic artery and portal vein will decrease simultaneously, with the proportion of the hepatic artery flow to the total liver inflow remaining essentially at 20%. The discussion indicates that, the hemodynamic environmental changes induced by liver injury provide a basis for the development of cardiac dysfunction, such as cirrhotic cardiomyopathy, and complement the traditional theory of metabolic abnormalities to some extent. The findings offer hemodynamic evidences for understanding how liver injury leads to changes in cardiac function and hold certain clinical significance.
-
Key words:
- liver injury /
- cardiac dysfunction /
- hemodynamics /
- in vitro simulated circulatory system
-
表 1 主要动脉分支的血流量分配比例
Table 1. Blood flow distribution ratios of major arterial branches
vessel name diameter/mm flow distribution ratio/% ascending aorta (inlet) 30.5 100.0 brachiocephalic trunk 12.7 11.8 left common carotid artery 7.2 2.9 left subclavian artery 9.6 6.5 celiac trunk 8.9 15.0 superior mesenteric artery 7.5 13.7 inferior mesenteric artery 4.0 2.1 left renal artery 5.6 13.5 right renal artery 5.6 12.8 left common iliac artery 12.0 11.0 right common iliac artery 12.0 10.7  下载: 导出CSV
下载: 导出CSV
-
[1] CONG F, ZHU L, DENG L, et al. Correlation between nonalcoholic fatty liver disease and left ventricular diastolic dysfunction in non-obese adults: a cross-sectional study[J]. BMC Gastroenterology, 2023, 23(1): 90. doi: 10.1186/s12876-023-02708-4 [2] WIJARNPREECHA K, ABY E S, AHMED A, et al. Evaluation and management of extrahepatic manifestations of nonalcoholic fatty liver disease[J]. Clinical and Molecular Hepatology, 2021, 27(2): 221-235. doi: 10.3350/cmh.2020.0239 [3] DUELL P B, WELTY F K, MILLER M, et al. Nonalcoholic fatty liver disease and cardiovascular risk: a scientific statement from the American heart association[J]. Arteriosclerosis, Thrombosis, and Vascular Biology, 2022, 42(6): e168-e185. [4] 许耀珑, 赵佳欣, 杨立刚. 非酒精性脂肪性肝病流行现状及危险因素研究进展[J]. 中国全科医学, 2024, 27(30): 3825-3834.XU Yaolong, ZHAO Jiaxin, YANG Ligang. Epidemic status and risk factors of non-alcoholic fatty liver disease[J]. Chinese General Practice, 2024, 27(30): 3825-3834. (in Chinese) [5] LUO J, XU L, LI J, et al. Nonalcoholic fatty liver disease as a potential risk factor of cardiovascular disease[J]. European Journal of Gastroenterology & Hepatology, 2015, 27(3): 193-199. [6] GONG H, LIU X, CHENG F. Relationship between non-alcoholic fatty liver disease and cardiac arrhythmia: a systematic review and meta-analysis[J]. The Journal of International Medical Research, 2021, 49(9): 3000605211047074. doi: 10.1177/03000605211047074 [7] M∅LLER S, HENRIKSEN J H. Cardiovascular complications of cirrhosis[J]. Gut, 2008, 57: 268-278. doi: 10.1136/gut.2006.112177 [8] HALLSWORTH K, HOLLINGSWORTH K G, THOMA C, et al. Cardiac structure and function are altered in adults with non-alcoholic fatty liver disease[J]. Journal of Hepatology, 2013, 58(4): 757-762. doi: 10.1016/j.jhep.2012.11.015 [9] YANO M, KOHNO M, KOBAYASHI S, et al. Influence of timing and magnitude of arterial wave reflection on left ventricular relaxation[J]. American Journal of Physiology-Heart and Circulatory Physiology, 2001, 280(4): H1846-H1852. doi: 10.1152/ajpheart.2001.280.4.H1846 [10] LATHAM R D, WESTERHOF N, SIPKEMA P, et al. Regional wave travel and reflections along the human aorta: a study with six simultaneous micromanometric pressures[J]. Circulation, 1985, 72(6): 1257-1269. doi: 10.1161/01.CIR.72.6.1257 [11] GUROVICH A N, NICHOLS WW, BRAITH R W, et al. Patients with refractory angina have increased aortic wave reflection and wasted left ventricular pressure energy[J]. Artery Research, 2014, 8(1): 9-15. doi: 10.1016/j.artres.2014.01.003 [12] QUAIL M A, SHORT R, PANDYA B, et al. Abnormal wave reflections and left ventricular hypertrophy late after coarctation of the aorta repair[J]. Hypertension, 2017, 69(3): 501-509. doi: 10.1161/HYPERTENSIONAHA.116.08763 [13] ADAMS L A, ANSTEE Q M, TILG H, et al. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases[J]. Gut, 2017, 66(6): 1138-1153. doi: 10.1136/gutjnl-2017-313884 [14] MATTHYS K S, ALASTRUEY J, PEIRÓ J, et al. Pulse wave propagation in a model human arterial network: assessment of 1-D numerical simulations against in vitro measurements[J]. Journal of Biomechanics, 2007, 40(15): 3476-3486. doi: 10.1016/j.jbiomech.2007.05.027 [15] REZAIENIA M A, PAUL G, AVITAL E J, et al. In-vitro investigation of the hemodynamic responses of the cerebral, coronary and renal circulations with a rotary blood pump installed in the descending aorta[J]. Medical Engineering & Physics, 2017, 40: 2-10. [16] XIAO N, ALASTRUEY J, ALBERTO FIGUEROA C. A systematic comparison between 1-D and 3-D hemodynamics in compliant arterial models[J]. International Journal for Numerical Methods in Biomedical Engineering, 2014, 30(2): 204-231. doi: 10.1002/cnm.2598 [17] CHEN D, LIANG S, LI Z, et al. A mock circulation loop for in vitro hemodynamic evaluation of aorta: application in aortic dissection[J]. Journal of Endovascular Therapy, 2022, 29(1): 132-142. doi: 10.1177/15266028211034863 [18] ERDOGAN D, BUSCH O R, VAN DELDEN O M, et al. Splenic artery Doppler waveform pattern in patients with cirrhosis and portal hypertension. [J]. Journal of Ultrasound in Medicine, 2006, 25(4): 453-459. [19] NAKAMURA M, KIDO M, TANIGAWA N, et al. Ultrasonographic assessment of hepatic artery and portal vein hemodynamics in healthy adults. [J]. Journal of Medical Ultrasonics, 2019, 46(3): 321-328. [20] 中国门静脉高压联盟, 中华医学会消化病学分会微创介入协作组. 中国肝静脉压力梯度临床应用专家共识(2023版)[J]. 中华医学杂志, 2023, 103(48): 3885-3895.Chinese Portal Hypertension Alliance (CHESS), Minimally Invasive Intervention Group, Chinese Society of Gastroenterology, Chinese Medical Association. Consensus on clinical application of hepatic venous pressure gradient in China (2023 edition)[J]. National Medical Journal of China, 2023, 103(48): 3885-3895. (in Chinese) [21] WANG Y, SHEN P, ZHENG M, et al. Influence of impeller speed patterns on hemodynamic characteristics and hemolysis of the blood pump[J]. Applied Sciences, 2019, 9(21): 4689. doi: 10.3390/app9214689 [22] IWAKIRI Y, TREBICKA J. Pathophysiology and management of portal hypertension[J]. Clinical Liver Disease, 2021, 17(3): 145-150. [23] YUMUSAK O, DOULBERIS M. Update on cirrhotic cardiomyopathy: from etiopathogenesis to treatment[J]. Annals of Gastroenterology, 2024, 37: 1-11. [24] FEDE G, PRIVITERA G, TOMASELLI T, et al. Cardiovascular dysfunction in patients with liver cirrhosis[J]. Annals of Gastroenterology, 2014, 27: 1-10. [25] M∅LLER S, HENRIKSEN J H. Cirrhotic cardiomyopathy: a pathophysiological review of circulatory dysfunction in liver disease[J]. Heart, 2002, 87(1): 9-15. doi: 10.1136/heart.87.1.9 [26] ZHANG J, LI Z, FENG L, et al. Hemodynamic impact of acute liver injury on cardiac function: an in silico study via a closed-loop cardiovascular model[J]. PLoS Computational Biology, 2026, 22(2): e1014006. doi: 10.1371/journal.pcbi.1014006 -

图(5) / 表(1)
计量
- 文章访问数: 116
- HTML全文浏览量: 45
- PDF下载量: 24
- 被引次数: 0

 渝公网安备50010802005915号
渝公网安备50010802005915号